
Antenatal Pathway
Antenatal Pathway
Screening for Trisomies in Pregnancy
Antenatal Diagnosis and Management of Trisomy 21 at Barnet Hospital
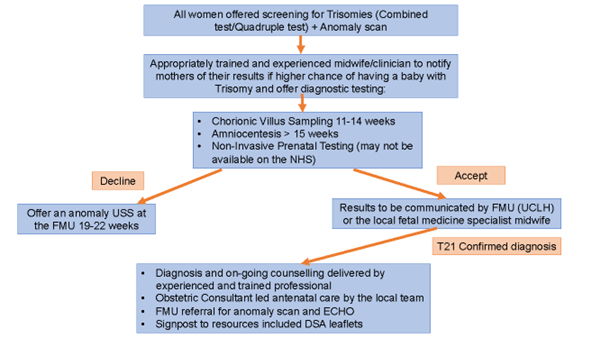
Diagnostic Testing Pathway:
CVS/Amniocentesis: Offered to women with a screen-positive combined or quadruple test, with appointments at UCLH Fetal Medicine Unit (FMU).
NIPT (Non-Invasive Prenatal Testing): Not provided at Barnet/Royal Free hospitals but may be offered at UCLH.
Communication of Results:
The FMU should communicate diagnostic results directly to the family and local fetal medicine specialist midwife.
A face-to-face appointment should be provided to discuss results with the local midwifery team.
Counselling should be delivered by trained professionals using the “Tell it Right” DSA training guide (Appendix 2).
Contacts:
Fetal Medicine Specialist Midwife: Mon–Fri, 8am–4pm
Tel: 0208 216 5140, Ext: 65140
Child Development Team (CDT): Available for family queries and introductions (Appendix 1 for details).
Resources for Families:
Antenatal Results and Choices (ARC): Website and helpline
Down’s Syndrome Association (DSA): Website and “Looking Forward to Your Baby” leaflet
Management of Pregnancy with Trisomy 21:
Risks:
Prematurity: Average gestation is 38 weeks.
CTG Anomalies: Continuous monitoring may be needed for growth restriction or identified risks.
Fetal Loss: Higher risk of miscarriage, stillbirth, and neonatal death.
Growth Monitoring:
Scans at 28, 34, and 38 weeks due to lower mean birthweight.
Fetal Movements:
Important: DS does not reduce fetal movements; reduced movements should always be investigated.
Hydrops and Transient Abnormal Myelopoiesis (TAM):
Hydrops Fetalis: A severe condition characterised by fluid accumulation in fetal compartments. It may indicate anaemia, often secondary to TAM, cardiac issues, or infection. Use MCA Dopplers to assess fetal anaemia.
TAM (Transient Abnormal Myelopoiesis): A pre-leukaemic disorder affecting up to 10% of neonates with DS, commonly presenting with hepatosplenomegaly, hydrops, or abnormal blood counts. Early diagnosis and close monitoring are critical as TAM can resolve spontaneously or progress to leukaemia. Delayed cord clamping should be avoided to reduce the risk of polycythaemia.
Structural Anomalies and Referrals:
Heart: Conduct fetal echocardiography due to a 40–60% risk of CHD.
Bowel: Polyhydramnios or bowel atresia requires referral to neonatal and surgical teams.
Brain: Mild ventriculomegaly often requires no further action if isolated.
Kidneys: Renal pelvis dilation should prompt referral to paediatric nephrology.